URINARY TRACT INFECTION IN KIDS
Urinary tract infection in kids(UTI) are quite common . The exact mechanism by which the enteric bacteria like E. coli, Bacillus proteus, Pseudomonas aeruginosa, Aerobacter aerogenes cause urinary tract infection is not known but in majority of cases it is an ascending infection from perianal or periurethral region.
During infancy, the ratio of UTI in male and female children is equal but after infancy it is 4 to 6 times more common in female children. The high rate of incidence in female children is mainly due to short urethra.

URINARY TRACT INFECTION IN KIDS
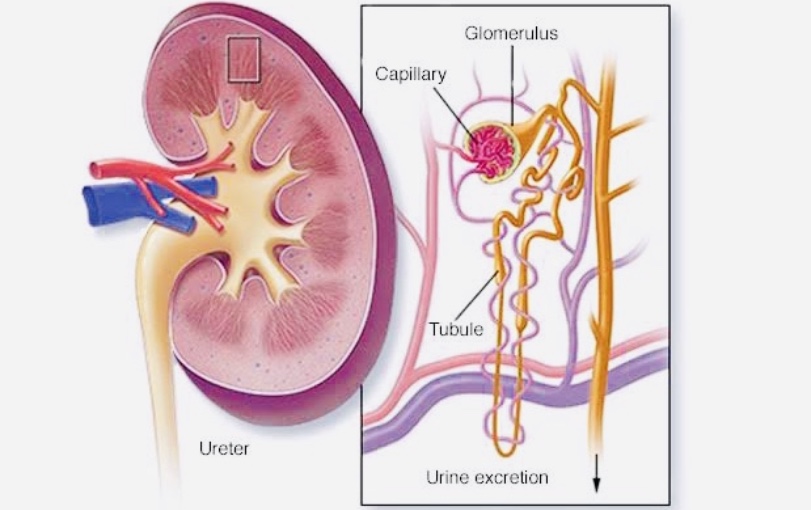
Pathogenesis of urinary tract infection in kids
During the first attack, the inflammatory changes are mainly in urinary bladder, causing the symptoms. Recurrent infec- tion may cause scarring of vesical smooth muscle and incompetence of vesico- ureteral valve leading to reflux of urine. This may spread infection to ureters and kidneys. In newborns and in septicemia involvement of kidneys may be due to he- matogenous spread. Vesicoureteral reflux is a congenital defect of vesicoureteral junction bilaterally or unilaterally causing recurrent UTI with renal scars.
Clinical Features Signs & Symptoms of urinary tract infection in kids
It may be asymptomatic and detected only after urine examination.
Urinary Symptoms
Frequency of micturition is increased (Polyuria), painful micturition (dysuria), burning micturition, urgency of mictu- rition, nocturnal enuresis, day time incontinence in previously dry child, foul smelling urine, rarely hematuria and oliguria may occur.
Other Symptoms of urinary tract infection in kids
Fever with chills. High fever without any signs. Fever may be associated with pain in abdomen and vomiting. There might be purulent discharge from urethral opening with redness over glans penis. On examination there might be tender- ness in suprapubic region. In recurrent urinary tract infection, with kidney involvement patient may have tender- ness in loin and renal angle.
Differential Diagnosis of urinary tract infection in kids
1. Causes of fever with chills a. Malaria b. Amebic hepatitis
2. Causes of dysuria, hematuria, oliguria
a. Acute glomerulonephritis
b. Urinary calculus
Investigations
1. Urine Examination
Urine may be alkaline if infectionis due to B. Proteus. Urine albumin is trace to + 1. Microscopic exam- ination: Pus cells more than 5 per high power field. Few RBCS may be present. Casts are absent in lower urinary tract infection. Bacteria may be present.
2. CBC
During acute stage, there might be leukocytosis with increase in neutrophil.
3. Urine Culture and Antibiotic Sensitivity
In grown up children, midstream sample is collected in a sterile container. The genital properly with mild antiseptic solution before collecting urine sample. The sample is immediately utilized for dip slide culture method. In small children sterile container is attached to external genital to collect the urine sample. cleaned Colony count more than 105 is significant. Repeat urine culture is done if count is between 103 and 105. Antibiotic sensitivity is done to know the appropriate antibiotic sensitivity.
4. Other Investigations
These are done when there is a history of recurrent urinary tract infection. These are mainly done to know the involvement of kidneys, anomalies of urinary tract, and to rule out urinary calculus.
you can read this also–https://medium.com/@rishu8565072311/common-cold-in-pediatrc-age-group-876172989cd2?source=friends_link&sk=690baac20ced0950d0126a694b383552
These investigations are-
a. Plain X-ray abdomen for KUB
b. Intravenous Pyelogram (IVP) – in children above 3-4 years of age
C. Ultrasonography of urinary tract
d. Micturating cystourethrogram
Complications
1. Recurrent and resistant urinary tract infection with vesicoureteral reflux of severe grade can cause renal scars and chronic renal failure.
2. Pyelonephritis
3. Failure to thrive
These complications occur due to re- current urinary tract infection.
Treatment of urinary tract infection-
Aim of the treatment is to- Eradicate the infection Prevent the recurrence
1. Advise patient to have plenty of fluids. To void urine at regular intervals to prevent stasis of urine. 2. Anti-bacterial therapy: Tab Cotrimoxazole: 6-8 mg of trimethoprim/kg/day in two divided doses for 2 weeks.
NOTE- Do not follow any treatment And medicine provided here ,please consult nearest hospital and talk to your doctor.This artical is only for knowledge purpose.
Team-Dailyayurvedic
Thank you